Your knee hurts. Stairs are hard, you've been told you may need surgery, the MRI makes you anxious — you can start a conversation from that stage. Knee pain is not decided by cartilage alone. We organize your MRI, X-ray, bloodwork, gait, and history, and confirm the next options with a physician. Together we sort out which option fits you: rehabilitation, orthopedic referral, watchful follow-up, or autologous adipose-derived MSC. We don't recommend MSC to everyone — which is exactly why, if it fits, you can move to the next step with confidence.
Entry: Knee suitability evaluation (3T MRI + physician review) / about one day in Ginza / fees are quoted individually at the physician consultation (private-pay). Share your records by LINE or email before your visit.
Self-pay (out-of-pocket) care · Screening, not a confirmed diagnosis · Individual results vary · MSC therapy is filed under Japan's Act on Safety of Regenerative Medicine and offered only to selected cases under physician judgment.
Knee pain is not decided by cartilage alone. We organize your MRI, X-ray, bloodwork, gait, and history, and confirm the next options with a physician. Even if your records are incomplete, you can start a reception consultation via your channel.
Your records don't need to be complete. Starting with whatever you have, you can begin a reception consultation via LINE or WhatsApp.
We organize what the MRI / X-ray shows. Imaging alone does not finalize a diagnosis or treatment plan.
We read the background of pain and swelling alongside lab data. Lab values alone do not decide eligibility.
We organize where any already-proposed treatment or surgery fits. When needed, consultation with a specialist or your primary doctor is a premise.
A physician confirms whether MSC and similar options could be a candidate. It is not suitable for all knee pain.
Based on the records, a physician organizes which options to consider.
Knee pain rarely has a single cause. Cartilage damage, meniscal injury, ligament problems, chronic inflammation, and advanced joint-space narrowing often coexist. The suitability of MSC therapy cannot be determined without an MRI and an integrated physician review.
Cartilage, meniscus, ligaments, synovial inflammation, osteophytes, and joint-space narrowing often coexist behind a single complaint of knee pain. Imaging anchors the assessment.
In Grade 4 (bone-on-bone) advanced osteoarthritis, orthopedic surgery or joint replacement may be more appropriate than MSC. Regenerative medicine is not the answer for every knee.
When MSC is not appropriate, CFO recommends rehabilitation, observation, or orthopedic referral candidly. Saying no is part of practicing regenerative medicine responsibly.
High-resolution 3T knee MRI is performed at Medical Scanning Ginza, within walking distance of CFO. The setup makes it practical to consolidate imaging, reading, and physician consultation during a short Tokyo stay.
According to OECD data, Japan ranks among the top countries by MRI units per capita. Central Tokyo offers practical scheduling for international patients with limited stay durations.
Note: Imaging infrastructure availability does not promise diagnostic or treatment outcomes. Final decisions are made through physician consultation and, where appropriate, referral to specialist medical institutions.
Knee MRI findings only inform an MSC suitability decision when integrated with symptoms, prior treatments, medication, metabolic context, and oncologic history.
Grades 1-4 organized using established frameworks (e.g., Kellgren-Lawrence) to clarify the boundary between regenerative and surgical care.
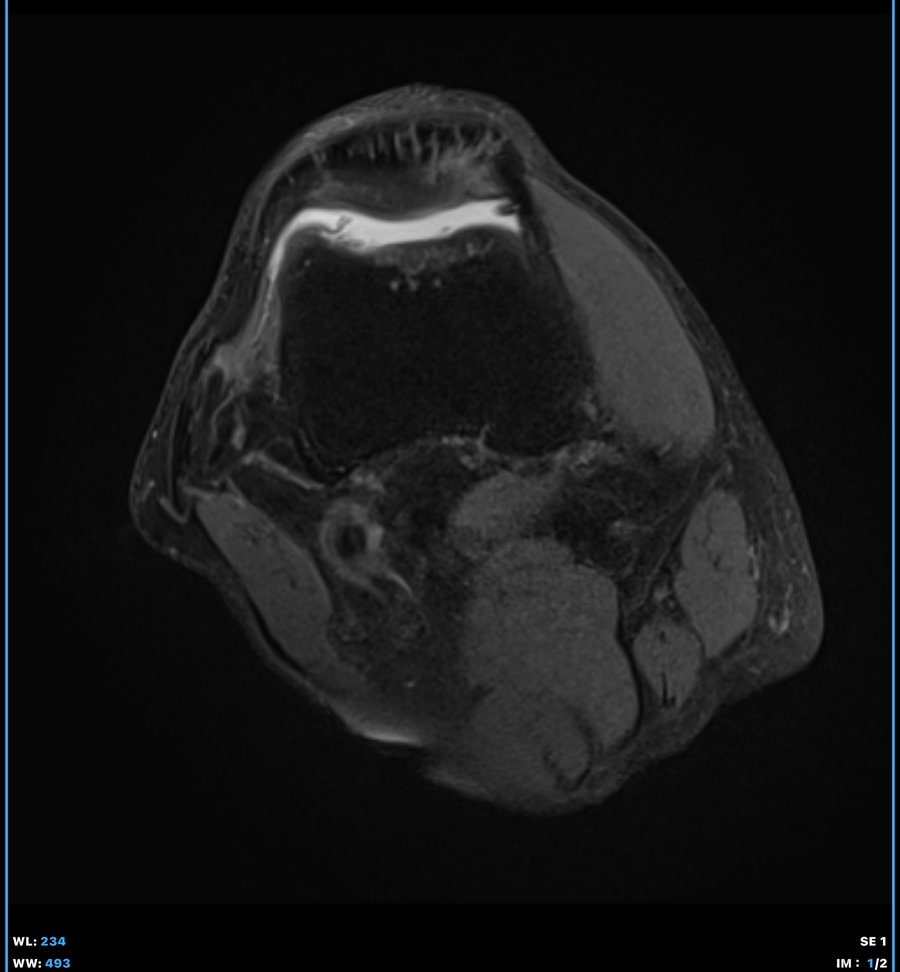
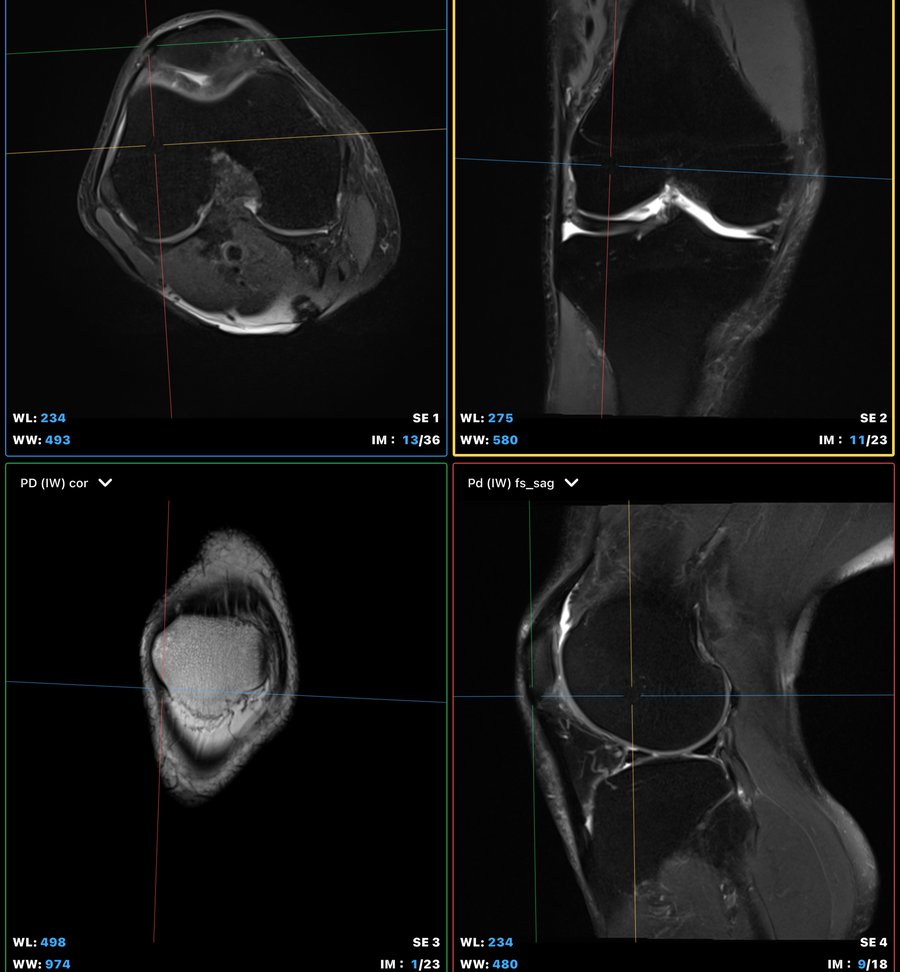
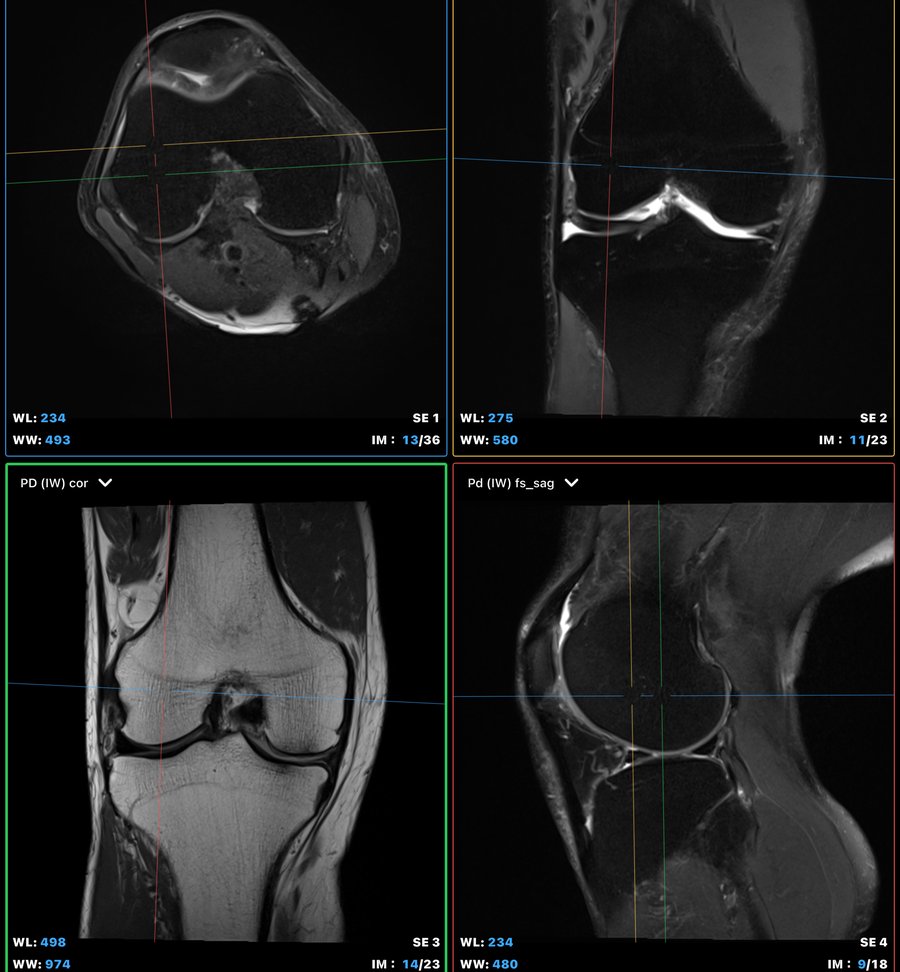
Femoral, tibial, and patellar cartilage thickness, defects, and focal lesions assessed on 3T MRI.
Medial / lateral meniscal tears and degenerative findings — important triggers for orthopedic referral when present.
Ligaments, synovium, joint capsule, bone marrow edema, cysts, and osteophyte status.
Pain, walking distance, range of motion, night pain, and stair tolerance.
Prior surgery, previous joint injections, current analgesics, supplements, and anticoagulants.
BMI, glycemic status, and chronic inflammation markers as contributors to joint load.
A history of cancer treatment or autoimmune disease requires especially careful physician judgment regarding MSC suitability.
Based on MRI findings and clinical assessment, the physician organizes the case into MSC candidate, orthopedic referral, observation, or further evaluation.
| Finding | Likely path |
|---|---|
| Grade 1-2 OA early cartilage change |
Rehabilitation, inflammation control, lifestyle guidance. MSC consultation possible but not required. |
| Grade 2-3 OA persistent symptoms |
After MRI and physician assessment, autologous adipose-derived MSC suitability review may be considered for selected patients. |
| Grade 4 / bone-on-bone joint space loss |
Orthopedic specialist or joint replacement discussion may be more appropriate. MSC alone is often insufficient at this stage. |
| Acute swelling · infection · trauma | Acute care first. MSC is postponed until the condition stabilizes and re-evaluation is completed. |
| Recent cancer treatment | MSC suitability requires especially careful physician review, considering oncology and orthopedic input. Decisions are individualized. |
| Unclear findings · systemic factors | Precision Check is recommended for broader assessment of inflammation, metabolic, and vascular factors beyond the knee. |
Note: This is a decision framework. Final decisions are made individually based on physician consultation, imaging findings, and clinical course.
Only when imaging findings, symptoms, prior treatments, medication, metabolic context, and oncologic history collectively support the indication, autologous adipose-derived MSC therapy may be considered. This is positioned as a conditional follow-on to the suitability evaluation, not a sales-driven treatment offer.
Note: Provided under osteoarthritis MSC provision-plan frameworks filed under Japan's Act on Safety of Regenerative Medicine (plan numbers PB3240166 / PB3250155). Filing represents the establishment of a provision framework and is distinct from national endorsement of treatment effect. Individual results vary.
When the clinic does not recommend MSC, alternative pathways are made explicit from the start. Recommending regenerative medicine to everyone is not appropriate clinical care.
For Grade 1-2 OA or muscle weakness as a primary driver, rehabilitation and lifestyle guidance are usually preferred first.
When BMI, glycemic status, or chronic inflammation contribute to joint load, metabolic improvement can be the most effective route to relief.
When meniscal or osteotomy surgery should come first, CFO assists with preparation for referral to specialist institutions.
For Grade 4 / bone-on-bone presentations, total knee arthroplasty discussion may be the realistic option.
When no immediate intervention is warranted, Monthly Review or Annual Re-Check is offered for monitoring.
If findings are not explained by knee pathology alone, Precision Check organizes inflammation, vascular, and metabolic factors.
CFO never administers MSC on the day of imaging. When MSC is considered, evaluation and any subsequent steps are planned individually by the physician, with details and timing determined on a case-by-case basis.
Share medical records, symptoms, and prior imaging via LINE / WhatsApp / email. Evaluation strategy is organized in advance.
3T knee MRI · physician consultation · OA grade review · suitability discussion. If selected and consented, the next steps are planned individually.
Autologous adipose-derived MSC is quality-reviewed at the partner CPC. No travel is required during this period.
After physician re-evaluation and final consent, any treatment is provided with details determined individually by the physician. Follow-up timing is determined individually.
Note: Travel schedule and stay duration are arranged individually. If suitability is not supported, subsequent steps are not performed. MSC is provided only after physician judgment, informed consent, and quality review.
Continued follow-up after MSC therapy or evaluation is supported, with timing determined individually by the physician. The physician team tracks pain, walking, rehabilitation adherence, and symptom progression.
Pain score, walking distance, range of motion, and medication status. Repeat imaging where appropriate.
Health-data organization and periodic review by the physician team. A monthly subscription option for patients seeking continuity.
Yearly repeat imaging and physician consultation. Next-action design adjusted to lifestyle and symptom changes.
No. The clinic first evaluates whether MSC therapy should be discussed. If MSC is considered, evaluation, quality review, informed consent, and any subsequent steps are planned individually by the physician. The clinic does not administer MSC on the day of imaging.
A specific outcome is not promised. MSC may be considered for selected cases where imaging and physician assessment suggest a reasonable regenerative medicine pathway. Advanced bone-on-bone disease may be better suited to orthopedic surgery or joint replacement. Individual results vary.
Knee pain can come from cartilage damage, meniscus injury, ligament issues, inflammation, or advanced joint narrowing. Offering MSC without imaging-based triage is not proper regenerative medicine. MRI helps determine whether MSC, rehabilitation, orthopedic referral, or observation is the most appropriate next step.
CFO will explain why and may recommend rehabilitation, observation, additional testing, orthopedic specialist referral, or joint replacement discussion. Not every patient should receive regenerative medicine. Honest referral is part of CFO's role.
EV / exosome treatment is not included in this knee front-door pathway. The clinic does not provide same-day cosmetic exosome treatment or allogeneic EVs. Autologous MSC-derived EV may be considered only after the patient's own MSC has been harvested, processed, and banked.
Yes. Patients may share medical records and prior imaging before travel via LINE, WhatsApp, or email. Diagnosis and treatment decisions are made through physician consultation. Multilingual pre-arrival consultation is available.
Patients currently undergoing or recently completing cancer treatment require special physician review before MSC suitability can be considered. Decisions are made individually under physician judgment, taking into account input from the treating oncologist and orthopedic specialist.
Before your visit, a short pre-consult (LINE / email) reviews your symptoms, history, and any prior imaging; then a 3T knee MRI evaluation helps you and the physician organize the option that fits you — rehabilitation, orthopedics, follow-up, or autologous adipose-derived MSC. This is not a treatment application; it is the entry point to find the right next step. Fees are quoted individually at the physician consultation (private-pay).
Domestic patients may prefer LINE; international patients typically use WhatsApp.